
Autoimmune thyroiditis, also known as Hashimoto’s thyroiditis (HT), is the leading cause of hypothyroidism. The disease is characterized by the presence of specific immune responses against the thyroid gland. These usually manifest as increased serum levels of thyroid tissue antibodies, i.e. antibodies to thyroid peroxidase (TPOAb) and thyroglobulin (TGAb) (1). Plasma antibody levels are positively associated with the severity of thyroid inflammation and hypothyroidism (2), but there is no specific treatment to reduce the antibody levels. Approximately 10-15% of the Australian population have positive thyroid antibodies, most commonly TPOAb, with a higher prevalence in women than men (3).
The essential biological action of vitamin D is regulation of calcium and phosphorus metabolism and preserving bone health. Vitamin D has also recently been shown to act in immune and endocrine regulation (4,5), and, accordingly, vitamin D deficiency was uncovered as a risk factor for autoimmune thyroid diseases, although the underlying mechanisms are still unknown (6).
Vitamin D deficiency is a worldwide public health concern. A recent study in Australia found that 17% of adolescents and 32% of young adults were vitamin D deficient (7). Risk factors for vitamin D deficiency include aging, female sex, winter season, obesity, malnutrition, lack of sun exposure, dark skin pigmentation and lower physical activity (7,8).
Epidemiological and clinical evidence
Research into the benefit of vitamin D in HT treatment and prevention has produced mixed results.
Vitamin D deficiency may be involved in the pathological mechanism underlying HT. Evidence indicates that vitamin D levels are significantly lower in patients with HT compared to healthy controls (9,10,11). The severity of vitamin D deficiency is associated with the duration of HT and thyroid antibody levels (12,13,14). However, conflicting results have been reported, with studies finding no relationship between vitamin D status and thyroid antibodies (15,16,17,18).
There is also only limited evidence of the effect of vitamin D supplementation for the prevention of HT. Results from a recent, large randomised controlled trial (almost 26,000 adults) found that supplementation for 5 years with vitamin D3 was associated with a 22% reduction in risk for confirmed autoimmune diseases, including autoimmune thyroid diseases (19). A case-control study found that each increase in serum vitamin D levels by 5 nmol/L is associated with a 1.62-fold reduction in HT risk (20).
The effect of vitamin D supplementation on immunity in patients with HT also remains inconclusive. Evidence indicates that vitamin D3 supplementation in individuals with HT decreases thyroid autoantibodies significantly, particularly if supplemented for more than 3 months, and in those who are vitamin D deficient, indicating that vitamin D treatment could delay the development of hypothyroidism (21). Other studies, however, found no significant effect on thyroid autoantibodies after supplementation with vitamin D in patients with HT (22,23,24).
A recent meta-analysis found that vitamin D supplementation might significantly increase the serum vitamin D levels and decrease TPOAb titres. No significant association was found between vitamin D supplementation and the levels of TGAb and thyroid hormones, thyroid-stimulating hormone (TSH), free triiodothyronine (FT3) and free thyroxine (FT4), suggesting that vitamin D is not associated with the function of the thyroid in patients with HT (25).
Serum TPOAb levels in HT patients were found to be significantly reduced after 4 months of vitamin D supplementation in HT patients (1,200-4,000 IU vitamin D3 per day, with the goal of vitamin D concentrations of up to 100 nmol/L) (26).
Mechanism of action
Vitamin D influences immunity by the production of anti-inflammatory and immune-regulatory markers via vitamin D receptor (VDR) expression in the nucleus of cells, stimulating innate and adaptive immune responses (27). As an active form of vitamin D, vitamin D3 integrates with VDRs to regulate calcium and phosphorus metabolism, control cell proliferation and differentiation and generate immunomodulatory effects (28). VDRs modulate the effects of vitamin D and polymorphisms of the VDR gene may decrease vitamin D activity (29). A significant link between VDR gene polymorphisms and autoimmune thyroid disorders has been reported in diverse ethnic groups (27).
Vitamin D may play an immunosuppressive role by inhibiting multiple parts of the HT immune response (22,30,31).
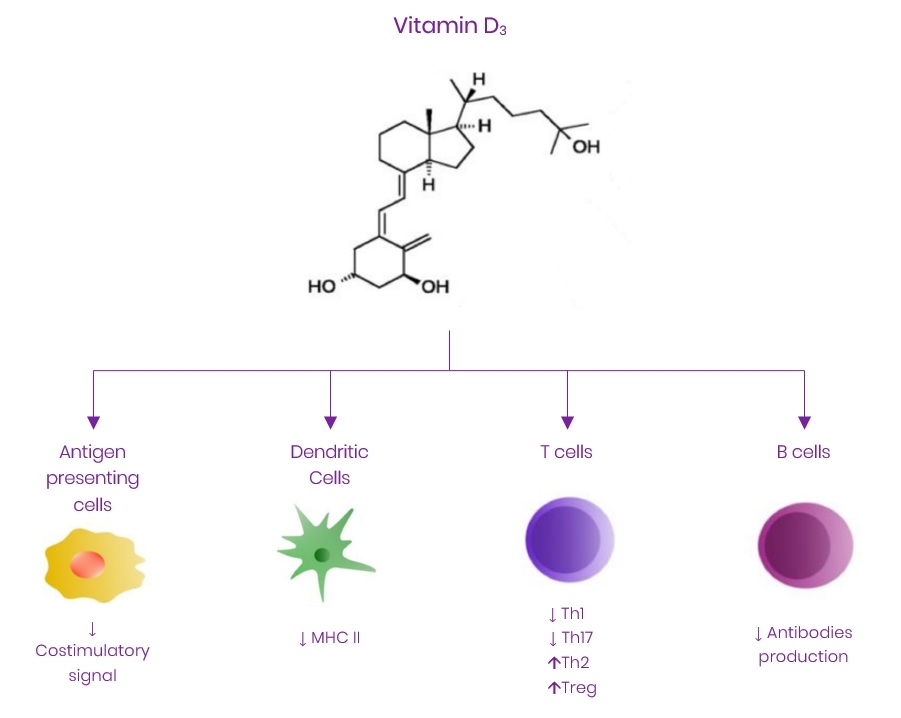
- Vitamin D promotes the metabolism of T regulatory (Treg) cells, diminishing T cell-dependent immune responses in autoimmune diseases (32,33). The reaction of T and B cells to thyroid antigens leads to HT in genetically vulnerable subjects (34).
- Vitamin D deficiency causes a large number of B cells to proliferate and differentiate into plasma cells, the latter secreting large amounts of immunoglobulins such as IgG and IgE, which eventually cause damage to thyroid cells and then trigger HT (35).
- T helper (Th1/Th2
 ) cell imbalance and Th1 cell activity enhancement are pathogenic factors of HT (36). Vitamin D inhibits HT by down-regulating the expression of the major histocompatibility complex class II (MHC II) stimulating molecules (CD40, CD80, CD86), increasing the production of interleukin-10 (IL-10) and reducing the secretion of IL-12, thereby repressing the Th1 cell immune response in the thyroid (37).
) cell imbalance and Th1 cell activity enhancement are pathogenic factors of HT (36). Vitamin D inhibits HT by down-regulating the expression of the major histocompatibility complex class II (MHC II) stimulating molecules (CD40, CD80, CD86), increasing the production of interleukin-10 (IL-10) and reducing the secretion of IL-12, thereby repressing the Th1 cell immune response in the thyroid (37). - Vitamin D inhibits differentiation of naïve T cells into Th17 cells and suppresses the secretion of Th17-derived cytokines IL-17 and IL-21, while promoting the metabolism of Treg cells to restore the balance of the body’s Th17/Treg cell ratio, and inhibit Th17 cell-induced thyroid inflammation (6).
Figure 1. Role of Vitamin D3 in regulating immune response. Adapted from (4) under CC BY 4.0
Limitations of studies
The nature of cross-sectional studies makes it impossible to draw a causal link between variables. In addition, there is a large degree of heterogeneity between studies, and results should be interpreted with caution. Heterogeneity in vitamin D studies results from:
- Differences in age, gender, study design, geographical variation, and quality of the studies.
- Seasonal variation in serum vitamin D levels is adjusted for in some studies but not all.
- Most studies disregard BMI as a confounding factor. The bioavailability of vitamin D diminishes with increasing BMI (38).
- Studies generally do not include information regarding dietary vitamin D intake that could affect serum levels of vitamin D.
- Inter-assay differences in the performance of commercially available kits for serum vitamin D measurement.
Conclusion
Epidemiological and clinical studies support an association between vitamin D and autoimmune thyroid disease. Vitamin D deficiency increases the risk of autoimmune thyroid disease. There is also some evidence supporting vitamin D supplementation to improve the condition of patients with autoimmune thyroid disease, however, given the heterogeneity of the study characteristics, a definitive conclusion remains elusive. Nonetheless, checking for and correcting any vitamin D deficiency in at-risk or diagnosed patients is a low cost and safe recommendation. If supplementation is required, vitamin D3 is preferable, administered for a minimum of 3 months. Overall, vitamin D could contribute to the prevention or correction of hypothyroidism and improvement of thyroid function, however, more research data are needed to verify the relationship between vitamin D deficiency and HT, which will help to determine whether vitamin D supplementation is effective for HT treatment.






