
Medicinal Cannabis
The cannabis plants Cannabis sativa and Cannabis indica, commonly called cannabis or marijuana, have been used for their psychotropic and mind-altering side effects for millennia. In recent years, there has been growing attention paid to the potential therapeutic benefits of cannabis.
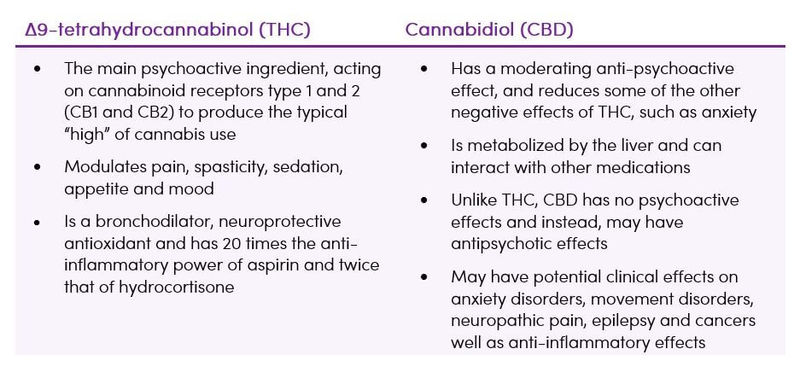
There are over 550 chemical compounds and over 100 phytocannabinoids isolated from cannabis, including Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD) (Table 1) (1).
Table 1. The main medicinal compounds in cannabis (1,2)
There are three main medicinal cannabis options, with differing laws and regulations regarding their use (3,4):
Raw herbal (botanical) cannabis
Any part of any plant of the genus Cannabis (most commonly C. indica, C. sativa and C. ruderalis).
Cannabis extract
Any extract, usually by organic solvents to produce oil, which is extracted from the plant, and any preparation consisting mainly of it. A magistral preparation is any medicinal product prepared in a pharmacy in accordance with a specified medical prescription for an individual patient.
Cannabinoids
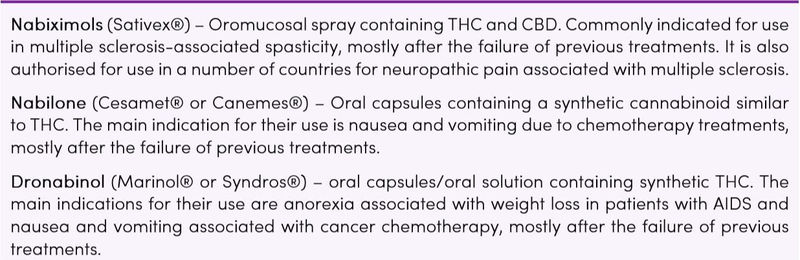
A class of chemical compounds affecting the cannabinoid receptors, with THC and CBD being the most commonly studied. Currently, there are only three synthetic cannabinoid-based medicines approved for use in different countries and recently available. They are not PBS registered in Australia (Table 2) (3).
Table 2. Pharmaceutical cannabis products (3)
Unregulated herbal cannabis is now available legally for medicinal use in much of the USA, but not Australia. It contains unknown concentrations of cannabinoids and potentially harmful impurities (4).
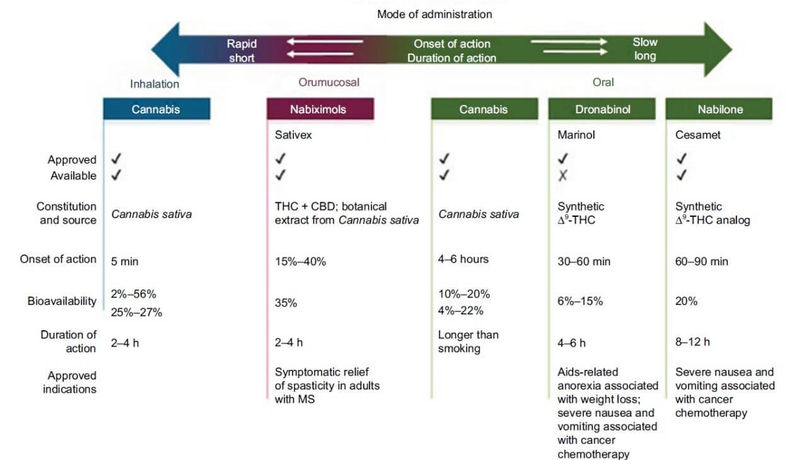
Figure 1. Mode of administration of THC (5) CC BY-NC 3.0
Some forms of medicinal cannabis are now available in Australia under the TGA’s Special Access Scheme, for use in exceptional clinical circumstances. Prescribers also need to comply with the State and Territory drugs and poisons legislation. Guidance documents on the use of medicinal cannabis are available from the Therapeutics Goods Administration (TGA) (6).
Smoking cannabis for medical purposes is not recommended. Many carcinogens are inhaled (as with tobacco), the dose is unpredictable and unregulated plant products are unlikely to be approved as medicines. Authorised prescribers in Australia can prescribe various forms of medicinal cannabis, such as oral solutions, oils, dried flower or capsules. These are in addition to the synthetic pharmaceutical products (Table 2) (7).
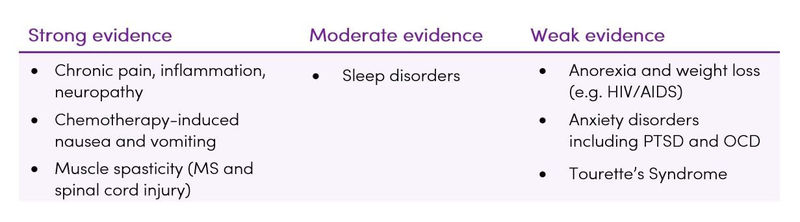
The major medical indications of medicinal cannabis are to relieve symptoms rather than cure a variety of diseases (Table 3) (8).
Table 3. Medical benefits of cannabis (8)
Traditional Understanding
Cannabis use has a long history of being used for medicinal purposes. Due to the illegal status of the plant, medicinal usage has not been regulated and the active ingredient dosages were unknown/inconsistent. The isolation of the major exogenous cannabinoid ligands THC and CBD a half-century ago accelerated research into therapeutic properties of cannabinoid signalling.
The Endocannabinoid System
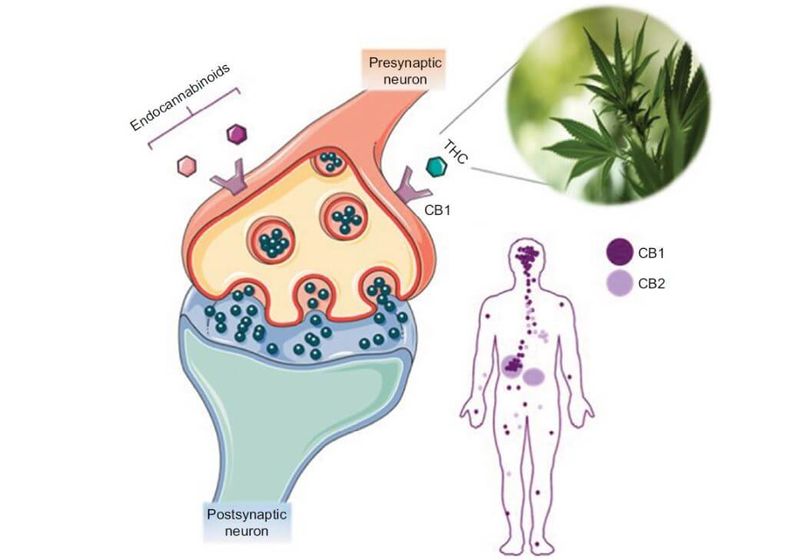
The endocannabinoid system (ECS) is a naturally occurring communication network that plays a role in many physiological processes. This system has been found to be implicated in many body systems and functions, including gastrointestinal function, appetite and metabolism, pain, memory, movement, immunity, inflammation, kidney disease and drug addiction (5,9,10). Cannabis and its component cannabinoids exert their effects primarily via the ECS (1).
The ECS includes receptors that bind cannabinoids, as well as a number of enzymes that facilitate their synthesis and degradation (1). The two G-protein-coupled receptors in the ECS are:
- Cannabinoid type 1 receptors (CB1) possess psychoactive potential and are expressed in the central nervous system (CNS), gastrointestinal system, adipocytes, liver tissue, and skeletal muscle. Due to their abundance in the body, particularly in the CNS, CB1 and its subsequent psychoactive effects have been extensively studied
- Cannabinoid type 2 receptors (CB2) are more restricted in their distribution and are primarily found on immune cells located in the tonsils, thymus, spleen, and bone marrow, as well as in the enteric nervous system within the GI tract (5). The CB2 receptor has a similar molecular structure to CB1 and activates overlapping downstream signalling pathways. The expression levels and patterns of CB2, however, are far lower than those of CB1, and the effects of CB2 activation do not include any that are psychoactive (11). CB2 receptor stimulation is associated with pain relief and anti-inflammatory activities but it is not associated with other CB1 effects such as appetite stimulation (2). CB2 is mainly expressed in the periphery under normal healthy conditions but may be upregulated in the CNS especially in conditions of disease or inflammation. CB2 is therefore expressed in the brain in unhealthy states (12)
Figure 2. The endocannabinoid system and CB1/CB2 distribution (5) CC BY-NC 3.0
Latest Research
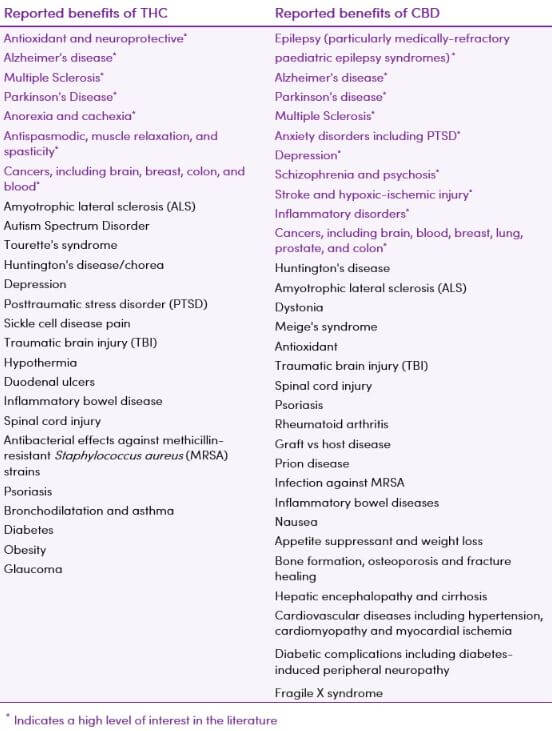
Both THC and CBD, as well as other cannabinoid molecules, are currently being evaluated for medicinal purposes, separately and in combination (Table 4) (1).
Table 4. Reported benefits of THC and CBD (13,14)
Neuropsychiatric Conditions
Research into the relevance of cannabinoids to diseases and their treatments has revealed a wide range of neuropsychiatric disorders that may be influenced by cannabinoid signalling (11,15). Results vary according to ligand and animal model for each neuropsychiatric disease.
Anxiety
Surveys suggest that over 50% of medical cannabis users are using it to reduce anxiety/stress (16,17).
THC increases the subjective effects of anxiety acutely in a 2-phase dose-related manner with lower doses producing decreases in anxiety and higher doses being anxiogenic. In contrast, CBD may have anxiolytic properties (1).
A dramatic decrease in anxiety has been demonstrated in adults using CBD. Improvements in anxiety persisted throughout the 3 month study (18).
CBD shows promise in reducing craving and anxiety in individuals with a history of heroin abuse, and may be a non-opioid option to help break the cycle of continued addiction (19).
Psychosis and Schizophrenia
Treatment of psychosis, including psychosis as a symptom of schizophrenia, currently addresses the positive symptoms through blockage of dopamine receptors but does not alleviate the negative symptoms or influence the symptoms' underlying neurobiological causes. CBD, on the other hand, leads to significant improvements in both positive and negative symptoms. The relationship between THC and CBD and psychosis is similar to that in anxiety; THC can induce schizophrenia-like symptoms such as psychosis and depersonalisation in high doses, but CBD has the capacity to somewhat reverse these effects (15,20,21).
For schizophrenia, there is early evidence that CBD may be a helpful treatment, while THC seems to worsen psychosis (5). Findings imply that not all people are affected equally by cannabis and heavy and early cannabis use is advised against.
Additional longitudinal research is needed to examine various levels of cannabis use on psychiatric symptoms and cognitive function with better control for confounding variables (5).
Alzheimer’s Disease (AD)
Individuals with AD have a significant reduction in CB1 receptor expression levels (11). Conversely, CB2 receptor expression in microglia and astrocytes are elevated. These findings, along with others, have fuelled the hypothesis that the ECS may have a neuroprotective influence, possibly stemming from its anti-inflammatory, anti-apoptotic mechanisms, as well as its neuromodulatory capacity (11). Experimental studies indicate that CB2 receptor activation counteracts the activation of microglia by amyloid β, and CB1 receptor activation is neuroprotective through a brain-derived neurotrophic factor-mediated mechanism (11).
THC has also been shown to treat symptoms of AD, such as agitation, if not the underlying causes (22).
Parkinson’s Disease (PD)
The ECS modulates dopamine signalling (11) and interestingly, the reverse is also true - imbalanced dopamine neurotransmission can also cause changes to endocannabinoid signalling. CB1 receptor levels are diminished in the basal ganglia, but not other brain regions in PD (23). Blocking CB1 receptor signalling in PD has yielded inconclusive results, however, cannabinoid signalling may yet prove to be influential in slowing PD progression. Research is now focusing more closely on factors such as CB1 antagonist dose, the type of neuronal injury occurring, and stage of disease progression, as well as possible roles for the CB2 receptor in microglia activation and inflammation that occurs in conjunction with neurodegeneration.
Studies collectively demonstrate that cannabis plays a role in improving quality of life measures in PD. Further studies are required to identify the exact effects/mechanisms of action (5).
Post-Traumatic Stress Disorder (PTSD)
There is much interest in the potential use of cannabis in individuals with PTSD, with frequent anecdotal reports of remarkable success. A recent case series reported on reduction in PTSD symptoms in adults with PTSD after administration of oral CBD in addition to routine psychiatric care (24). Ongoing clinical trials will hopefully provide more evidence on the effect of cannabis and cannabinoids (8).
Huntington’s Disease (HD)
Individuals with HD have a downregulation of CB1 receptors in affected brain regions, as well as upregulation of CB2 in microglia. Cannabinoid expression changes during the disease progression. CB1 antagonism exacerbates disease progression. Results of clinical trials using cannabinoids in HD have produced conflicting results (11).
Multiple Sclerosis (MS)
Clinical literature suggests that cannabinoids have demonstrated therapeutic effects for the treatment of auto-immune disorders, including MS (25,27,27).
The ECS may work to counteract symptoms of MS (11). There are indications that medicinal cannabis is effective in reducing patient-reported symptoms such as spasticity and pain, however, cannabinoids have no proven overall effect on the progression of MS (5).
Epilepsy
Cannabis has been known to hold anticonvulsant properties for more than a millennium, however, cannabis use for the treatment of seizures was not studied formally until the late 20th century (15).
Based on high-quality clinical trials there is evidence that CBD is effective on Lennox Gastaut, Dravet syndrome, and other types of childhood treatment-resistant epilepsy, with a low number of associated adverse events (5,28,29).
Sleep Disturbances
There is moderate evidence that cannabinoids, predominantly nabiximols, effectively improve the short-term sleep outcomes in individuals with sleep disturbances associated with obstructive sleep apnoea, fibromyalgia, chronic pain and multiple sclerosis (8).
Pain
The ECS is a critical endogenous pain control system and the targeting of this system with cannabis may provide a therapeutic advantage in the treatment of pain (30). The modulation of pain is thought to be due to inhibition of presynaptic neurotransmitter release and modulation of postsynaptic excitability (31,32).
The pain-relieving effects of cannabinoids have been demonstrated in clinical trials, specifically in chronic neuropathic pain (5,8,33).
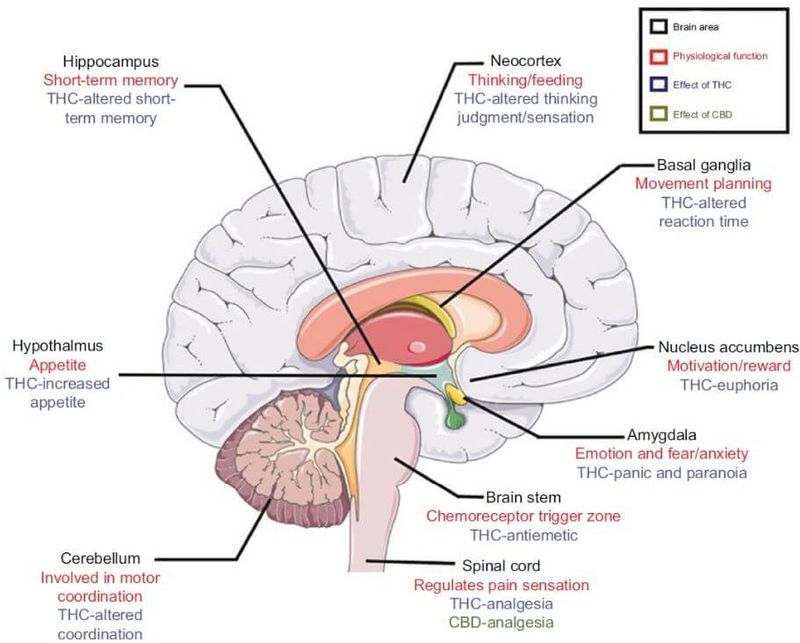
Figure 3. Effects of cannabis on the central nervous system (5) CC BY-NC 3.0
Gastrointestinal (GI) Disorders
The endocannabinoid system is vastly integrated within the GI tract, particularly within the enteric nervous system suggesting a potential therapeutic role for medicinal cannabis in GI disorders (5).
Nausea and vomiting
There is an abundance of anecdotal reports and accumulated clinical experience of the benefits of cannabis in reducing chemotherapy-related nausea and vomiting. A Cochrane review concluded that cannabinoids are highly effective, being more efficacious than the placebo and similar to conventional antiemetics in treating chemotherapy-induced nausea and vomiting (34).
Inflammatory Bowel Disease (IBD)
A significant portion of self-medicating IBD patients find cannabinoids (particularly THC) helpful for symptoms such as abdominal pain, poor appetite, nausea, diarrhoea and joint pain (5). There is, however, a lack of reliable clinical evidence to support the use of medicinal cannabis in the treatment of IBD.
Cancer
Cannabinoid compounds can reduce tumour growth in animal models of cancer. Increases in CB1 or CB2 expression have been observed in association with some cancers, and cannabinoids (endogenous and exogenous) have demonstrated an ability to combat cancer without harming the body's cells. Cannabinoids can slow the processes of cancer cell proliferation, metastasis, and angiogenesis (35).
The bulk of the substantial literature is preclinical and heavily focused on the effect of cannabinoids on gliomas. A review of experimental studies showed that cannabinoids selectively kill the glioma cells while leaving normal brain cells unharmed (36). Clinical data suggesting a benefit in people with cancer is lacking (8,37). An Australian trial is currently underway investigating the tolerability and effect of oral medicinal cannabis on quality of life in recurrent glioblastoma multiforme patients. This trial will also assess the effect of cannabis on glioma tumour growth (38).
There may be significant quality of life benefits, including decreased anxiety, pain, and depression and increased appetite and generalised feelings of well-being, associated with medicinal cannabis use among patients with newly diagnosed cancers (39). Currently, cannabinoids are used for palliative treatment of cancer patients, despite a low-quality of evidence (40).
Antioxidant and anti-inflammatory
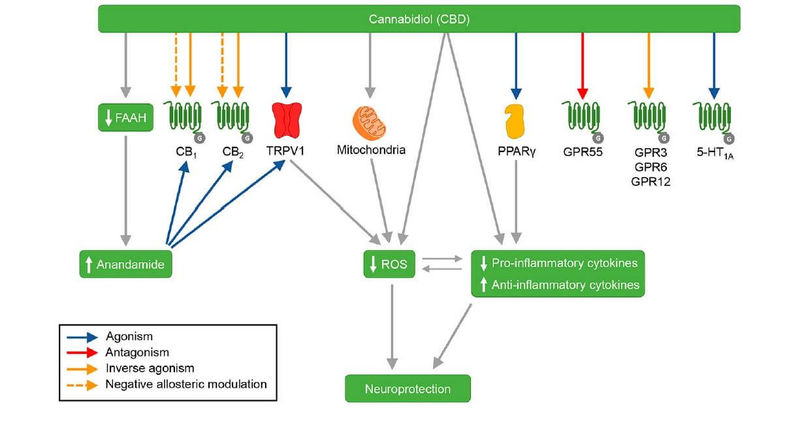
CBD exhibits anti-inflammatory and antioxidant actions (41). CBD treatment decreases the levels of pro-inflammatory cytokines and increases the levels of anti-inflammatory cytokines. CBD can also affect the expression of several genes involved in zinc homeostasis, which is suggested to be linked to its anti-inflammatory and antioxidant actions (42).
Figure 4. CBD’s mechanisms of action (42)
Takeaway on Medicinal Cannabis
- The endocannabinoid system (ECS) consists of ligands and receptors expressed widely in both the brain and periphery, where they act to maintain balance in a number of homeostatic processes
- The ECS can play a positive role in a wide range of conditions. Future research will hone therapeutic targets in each disease state. The major medical indications of medicinal cannabis are to relieve symptoms rather than cure a variety of diseases (8)
- A growing body of research supports the concept that CBD and TCH can improve causes and symptoms in a number of neuropsychiatric and neurodegenerative disorders
- CBD lacks the psychoactive effects associated with THC and, in general, is regarded as a safe compound (43)




